
Nutrition
Do You Need a Vitamin B6 Supplement and Can The Wrong Type Actually Cause A B6 Deficiency?

Vitamin B6 is one of the most popular vitamins found in supplements sold today, with between 28% and 36% of Americans using supplements containing B6 (1). There’s a good reason for this because it’s vital in a huge number of reactions in the human body. So if you’re taking a multivitamin, a joint care formula or a workout supplement there’s a good chance it contains B6, often in very high doses.
Table of Contents
Why Do You Need Vitamin B6?
For example, B6 is necessary for the metabolism of amino acids that make up all of the proteins in our body. These Amino Acids are also used to produce neurotransmitters such as Serotonin, Dopamine, and GABA. B6 also helps convert the amino acid Tryptophan into Nicotinamide which is then used in energy production and the recycling of antioxidants such as Glutathione in the body (2, 3, 4).
B6 is also needed for the production of Haemoglobin which transports oxygen in the blood (5), and Glycogen which is the storage form of energy in the muscles and liver. It’s also needed for gene expression (2, 3, 4).
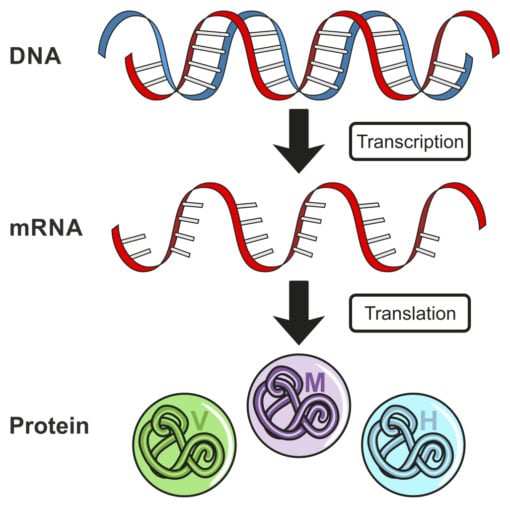
Gene expression is the process in which a protein is created from one of our 25,000 genes. Genes are a blueprint for creating proteins, and Genes are made up of DNA. Whether a gene creates a protein or not depends on the signals or a cell receives or the ‘environment’ that it’s exposed to. If a certain environment is created a gene will be expressed or ‘read’, and a protein will be made. B6 or a deficiency in B6 has been shown to increase, or sometimes decrease the expression of certain genes (4).
With all these metabolic functions dependant on having enough B6 then it’s hardly surprising that we find it in so many supplements. However, most normal diets generally provide the recommended daily allowance of B6, as it’s found in many different food types. The RDA of B6 ranges from 1.4 – 2.1 mg a day depending on age and sex, which is roughly what most people get from the food they eat if they are eating enough calories to maintain healthy body weight.
Why Is There a Need to Put B6 in so Many Different Supplements?
Well despite the fact that’s it’s readily available in the diet, many people actually show the signs of not getting enough B6! The reason is that there are a number of lifestyle-related issues that can stop us from either absorbing enough B6, using B6 efficiently in the body or significantly increasing our needs for B6.
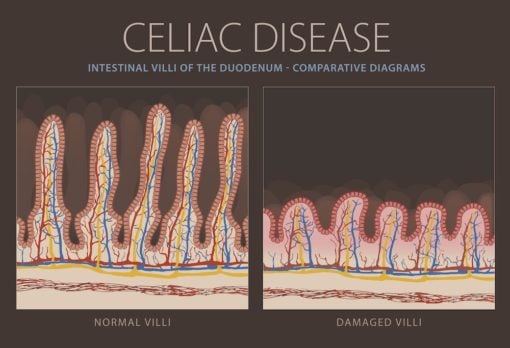
For example diseases such as Celiac Disease, Crohns and Colitis can stop people absorbing enough B6 (2, 5). However, these conditions involve significant damage to the gut, and so people don’t just wake up one day and instantly have one of them, they will normally take many years to develop. So just as the damage to the gut doesn’t begin when one of these diseases is diagnosed, neither does the reduced absorption of vitamins. That too will typically start years before a diagnosis.
So anyone with any digestive issues could have a reduced ability to absorb B6. Warning signs of this would include IBS symptoms including regular constipation or diarrhea, bloating after meals, Acid Reflux and excessive gas.
Diabetes, Alcoholism and the use of certain drugs (for example oral contraceptives) can reduce our ability to use B6 in cells (2, 4). And perhaps most relevant for people today stress and inflammation can also significantly increase our need for B6 (6).
Stress and B6 Vitamin Supplementation
Because stress is so common in the modern world, it means many of us are living with the evolutionary equivalent of a fire alarm going off in our body. Worrying about missing your train, picking up your children from school and making the mortgage payments next month is stressful. Throughout our evolutionary history stress was a short term thing, for example dealing with danger such as wild animals, but today it’s pretty much non stop.
Humans cope well with short term stress, in fact, it can often improve our health, this positive stress is known as eustress. However when it’s chronic, it causes prolonged low-level immune activation, and immune activation damages things including our own cells. That the immune system can damage things is useful when we need to kill a virus or other pathogen, however, when it’s just reacting to chronic stress it causes more harm than good.
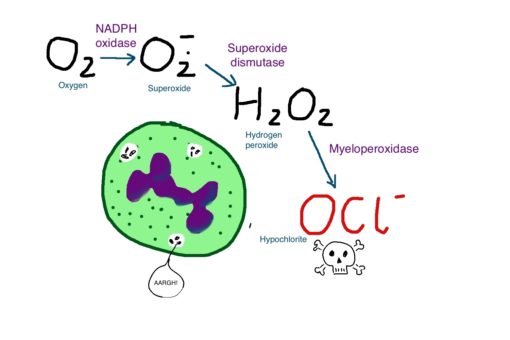
An example of how the immune system works is that it often uses hydrogen peroxide to kill off invaders. Hydrogen peroxide has another name and that’s household bleach. So just as bleach kills off the bad guys in our toilets, it does the same in our bodies. But in chronic low-level immune activation, the immune system is constantly firing bleach at our own cells, so it’s vital for the body to be able to effectively turn this off.
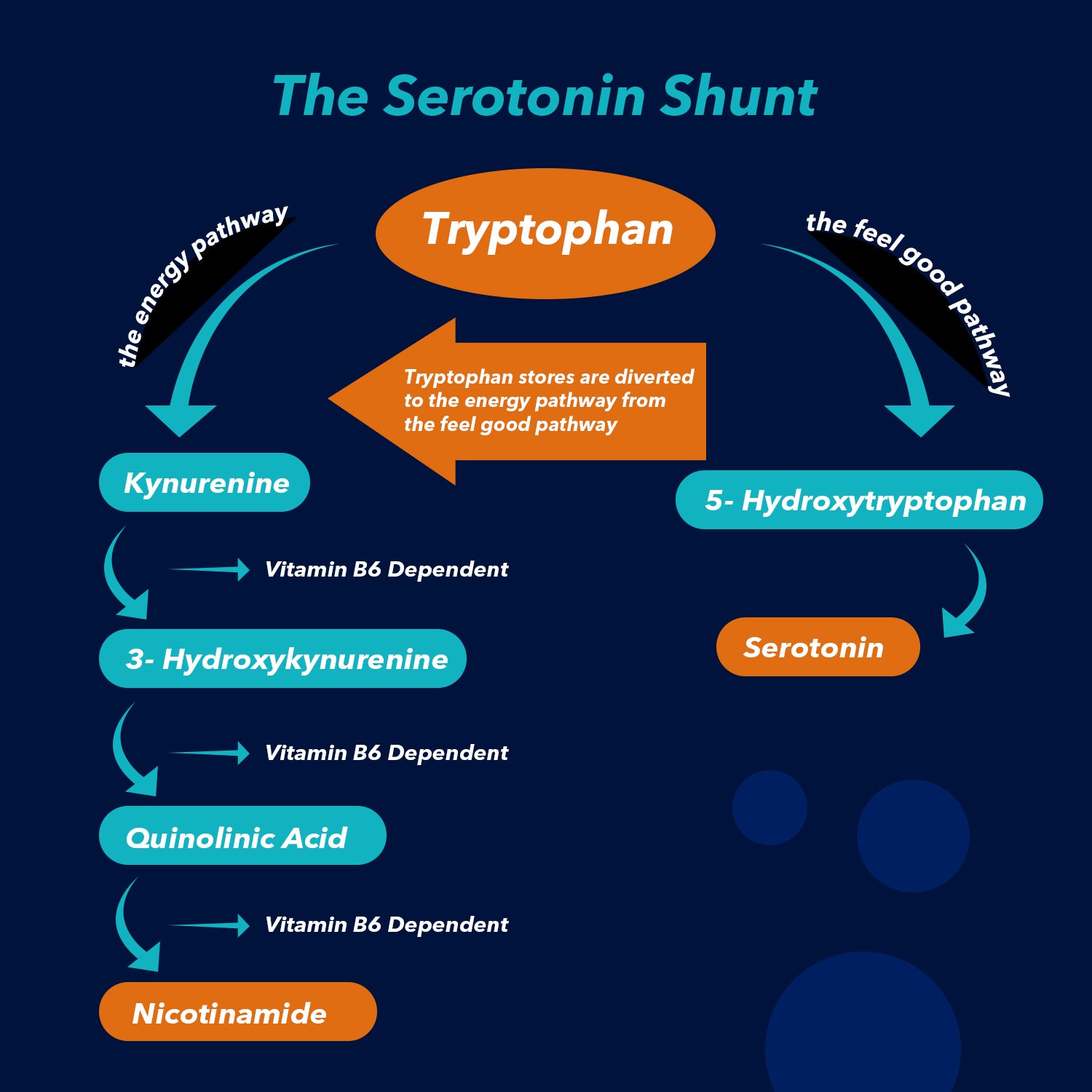
A key way that this can be done is through the production of Nicotinamide, through a pathway called the Kynurenine pathway. This pathway takes the amino acid tryptophan and turns it into Nicotinamide, and this conversion is dependant on vitamin B6 (2). Also, Nicotinamide is vital for energy production.
Stress or inflammation increases activity in this pathway so can easily increase the amount of B6 a person needs. As well as producing Nicotinamide, Tryptophan is also used to produce Serotonin, which is the ‘feel-good’ neurotransmitter, and the one most often thought to cause depression. If we have high levels of stress, Tryptophan can easily be diverted from producing Serotonin to producing Nicotinamide.
This change or “serotonin shunt” as it’s often referred to is a clear model of how stress can cause depression. Unfortunately, from an evolutionary point of view having the energy to escape that tiger, or at least the one our body has been tricked into thinking we’re escaping from due to chronic stress or inflammation, is more important to our survival than feeling good (7).
Stress also causes an increased breakdown of tissue in the body for energy production. Breaking down tissue like muscle for energy is useful when we’re running from a tiger, but it’s not so useful when we’ve braked too late on the commute home and dented the bumper on the car in front of us. Nevertheless, this increased breakdown of proteins require B6 to happen.
So really if you’re stressed or suffering from long term inflammation, and inflammation is involved in every chronic complaint humans suffer from today, from long term indigestion to autoimmune conditions, you may need more B6 than the current RDA.
So what are the signs of not getting enough B6?
Because it’s involved in so many different processes in the body if you are low on B6 you won’t be feeling great. It will commonly cause tiredness, irritability, and difficulty sleeping (3), as well as pain, weakness, and numbness in the legs and arms (4). These symptoms in the arms are known polyneuropathy which basically means damage to the nerves of the arms and legs.
More prolonged Vitamin B6 deficiency has also been associated with Cardiovascular disease (8), Stroke (9), Cancer (10) and cognitive decline in the elderly (11).
If you don’t want to guess whether any symptoms you are experiencing are due to low B6, you can get a B6 test done. For this I prefer a urine test, because red blood cell and blood plasma tests can be misleading as they don’t measure B6 activity in the cells. Urine tests measure a substance called Pyrodoxic acid which is excreted from the body in the urine, and is what B6 is broken down into in cells when it’s not used for metabolic processes. So if you get a low reading you know all your B6 is being used up by the cells and there is none left over to break down and excrete in the urine (2).
The Right Dose of B6 Vitamin
I Can’t be Bothered With a Test, I think I’ll Just Take a Supplement to be Safe!
The problem is that Vitamin B6 supplementation has been shown to actually cause symptoms of Vitamin B6 deficiency! Some people taking high doses of B6 long term were reporting pain and weakness in their arms and legs, aka the Polyneuropathy often found in people suffering from B6 deficiency (12, 13).
Say What?
As I mentioned at the beginning of this article, supplements often contain much higher doses of B6 than the recommended daily amount. This is because B6 has always been considered to be a safe supplement, with the excess in the body easily broken down and then excreted in the urine (14).
However, due to an increasing number of studies finding adverse symptoms with high doses of B6, the US Dietary Association (USDA) put an upper limit of 100mg per day of B6, and then more recently the European Food Safety Authority (EFSA) went further and established a maximum of 25mg a day.
But despite a recognition that large doses of B6 in supplements over the long term can cause problems, the question of why B6 was producing these paradoxical reactions still remained. Then in 2017, a study emerged that showed the answer (15). To understand what was happening, and how we can make sure we get the benefits from having enough B6 through supplementation and none of the potential problems, we need to understand a little bit about what B6 actually is.
B6 is Actually 6 Different Molecules
B6 has 3 main types called Pyridoxine, Pyridoxal, and Pyridoxamine, and those 3 types also have 3 more types where a phosphate molecule is added to them so Pyridoxine Phosphate, Pyridoxal Phosphate and Pyridoxamine Phosphate (2).
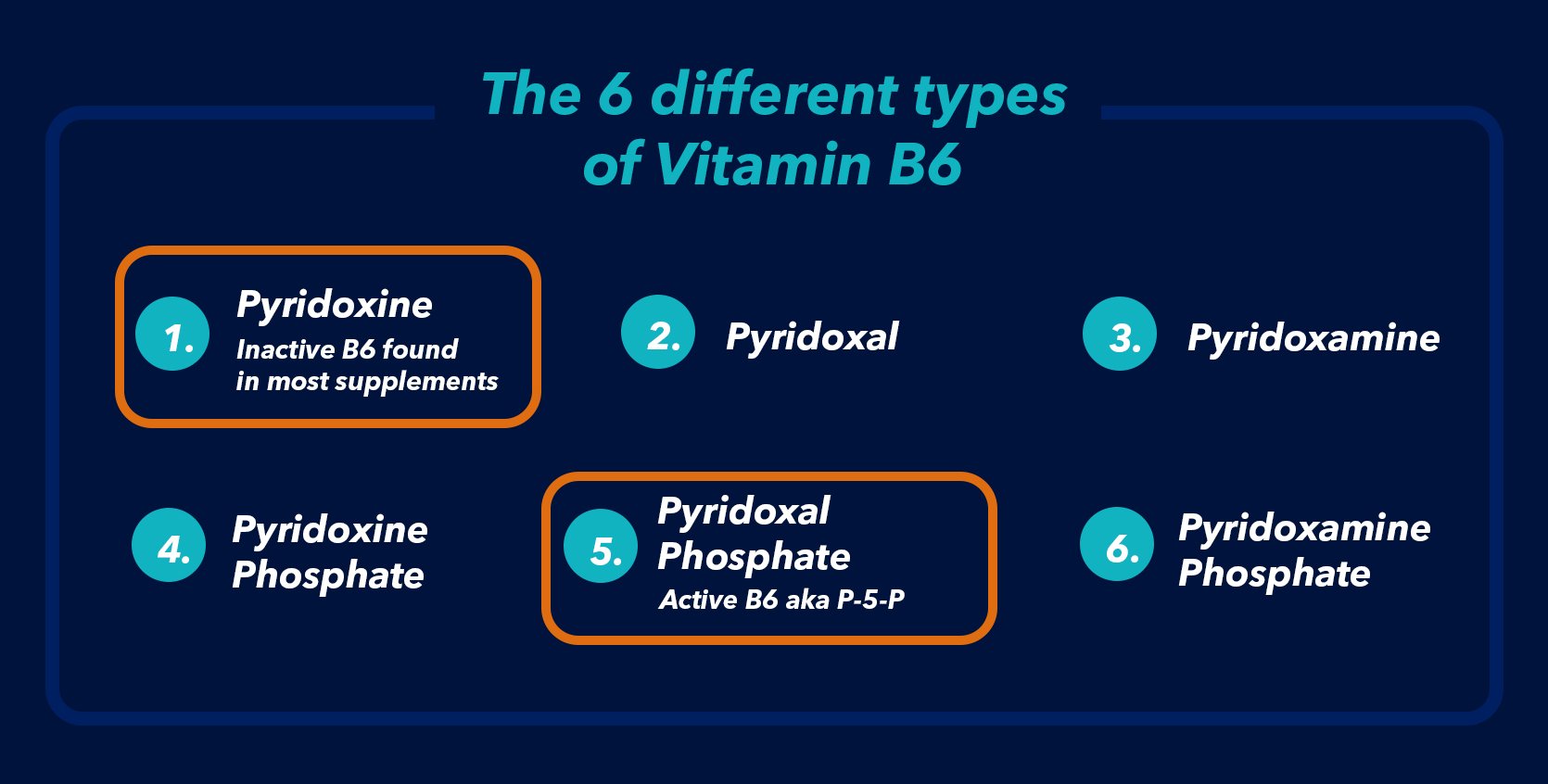
Although there are 6 different types, only 1 of those types is the active form of Vitamin B6 that is used as a co-factor for enzymes in the body. The Active type is Pyridoxal Phosphate, which is often abbreviated as P-5-P. The other forms have to be converted in the liver into P-5-P before they can be used by enzymes in the body.
This is where the problem is, in that the vast majority of supplements do not contain P-5-P, they actually contain the inactive form Pyridoxine. This was never seen as a problem because conversion can happen in the liver and any excess is passed out of the body in the urine.
However, the 2017 study tested P-5-P against Pyridoxine, to find out the effect it had on neuronal cells in a lab, at concentrations found in the body. Because Neuronal cells are very slow to multiply they used cancerous cells which multiply readily and exposed them to P-5-P and Pyridoxine. They found after 24 hours of exposure, pyridoxine significantly increased neuronal cell death, whereas P-5-P did not change the outcome from the control. They were also able to stop cell death by adding P-5-P to the cells exposed to Pyridoxine.
Pyridoxine Competes With P-5-P For Enzymes.
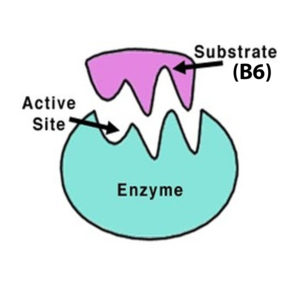
So we know they Pyridoxine on its own is bad news for cells, but why is that? The researchers went on to test the effects of both Pyridoxine and P-5-P on 2 different enzymes. An enzyme makes a reaction happen in the body, for example, it turns one amino acid into another. Vitamin B6 is a cofactor for some enzymes. You can think of B6’s role as a jigsaw puzzle piece. B6 slots into space on the enzyme and then the complex is complete and can do its job!
They used Tyrosine Decarboxylase which turns the amino acid Tyrosine into Tyramine, and also Alanine Transaminase, which transfers an amino group from alanine into α-ketoglutarate, to produce pyruvate and glutamate. Alanine Transaminase is most often used in Liver tests where it’s known as ALT. Both of these enzymes need B6 to function. In their experiment, Pyridoxine decreased the activity of these enzymes, whereas P-5-P increased them.
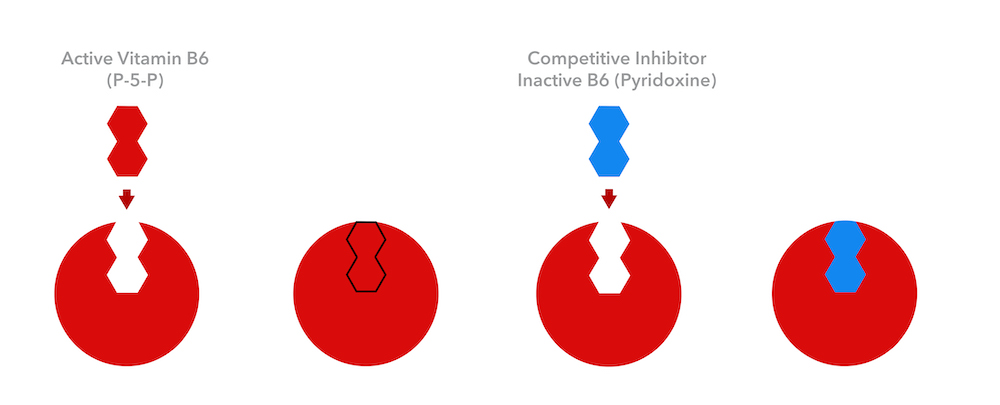
They were able to conclude that the reason Pyridoxine can cause problems for people is that it competes with P-5-P for the empty slot on the enzyme. They are both versions of Vitamin B6 which are almost identical, but not quite. That means Pyroxine can fit in the same hole as P-5-P, but once it’s in that hole it can’t make the enzyme do its job, because chemically it’s not quite correct. This is known as “Competitive Inhibition”. So the Pyridoxine is competitively inhibiting the P-5-P.
We can think back to the jigsaw puzzle example to get a clearer idea. Let’s say you’re finishing off a jigsaw picture of a red circle, (ok it’s not a very interesting jigsaw, but that doesn’t matter!), and you’re down to the last piece and you pop it in, but instead of the color of the final piece being red, it’s blue instead. The jigsaw is complete, but the picture is wrong.
So if you have Pyridoxine in a supplement, some of it will be converted to P-5-P, but also some will be in the cells competing with P-5-P for enzymes, which stops some of them working. In the case of the ALT enzyme, they will still be working in your body, but not as efficiently because the Pyridoxine will be attaching to some of the ALT enzymes instead of the P-5-P.
We know that doses of 25mg or 50mg of Pyridoxine, (the doses regularly found in multivitamins), can significantly increase blood plasma levels of Pyridoxine, so even if someone taking them is not experiencing numbness of weakness, enzyme efficiency could still be affected.
Then why do Most B6 Supplements Contain Pyridoxine and not P-5-P?
The main reason is cost, with P-5-P costing around 6-7 times as much as Pyridoxine, but also a lack of understanding amongst supplement companies that the difference between the two can actually cause problems for people taking their supplements. The good news is any pain or weakness that is felt when taking the inactive form Pyridoxine usually goes away quickly when a person stops taking it.
We recommend to prevent any issues and to ensure you’ve always got enough B6, to just using supplements and Multi-Vitamins that only contain P-5-P, with no Pyridoxine at all, and only take up to 25mg a day. This is easy to check when buying supplements, just take a look at the supplement facts panel in the images if you’re buying online, or on the back of the bottle if you’re in a store. It will clearly show what form the Vitamin B6 is in, just look for P-5-P or Pyridoxal Phosphate, anything that says Pyridoxine is the inactive form and is best avoided.
An example of a product that uses P-5-P is our very own nootropic stack, Seneca Nootropic. This product contains 18 research-backed ingredients, including 4mg of Vitamin B6 as P-5-P in every serving! Not sure what a nootropic is? Read our guide that details everything you should know about nootropics and cognitive enhancing supplements.
References
(1) Bailey RL, Gahche JJ, Lentino CV, Dwyer JT, Engel JS, Thomas PR, Betz JM, Sempos CT, Picciano MF. Dietary supplement use in the United States, 2003-2006. J Nutr. 2011 Feb;141(2):261-6. doi: 10.3945/jn.110.133025. Epub 2010 Dec 22.
(2) Per Magne Ueland, Arve Ulvik, Luisa Rios-Avila,Øivind Midttun,2 and Jesse F. Gregory3. Direct and Functional Biomarkers of Vitamin B6 Status. Annu. Rev. Nutr. 2015. 35:4.1–4.38
(3) Martino L. di Salvo, Martin K. Safo, Roberto Contestabile. Biomedical aspects of pyridoxal 5′-phosphate availability. Frontiers in Bioscience E4, 897-913, January 1, 2012
(4) Spinneker, A.; Sola, R.; Lemmen, V.; Castillo, M. J.; Pietrzik, K.; González-Gross, M. Vitamin B6 status, deficiency and its consequences – an overview. Nutrición Hospitalaria, vol. 22, núm. 1, enero-febrero, 2007, pp. 7-24
(5) Shane B. Folate, vitamin B12 and vitamin B6. In: Stipanuk MH, editor. Biochemical, physiological, molecular aspects of human nutrition, 2nd ed. New York: Saunders; 2006. pp. 693–732.
(6) Iwakawa H, Fukui T, Fukuwatari T, Bamba S, Sasaki M, Tsujikawa T, Doi Y, Shibata K. Blood concentrations and renal clearance of water-soluble vitamins in outpatients with ulcerative colitis. Biomed Rep. 2019 Mar;10(3):202-210
(7) Robert Dantzer, Jason C. O’Connor, Gregory G. Freund, Rodney W. Johnson, and Keith W. Kelley. From inflammation to sickness and depression: when the immune system subjugates the brain. Nat Rev Neurosci. 2008 Jan; 9(1): 46–56
(8) I. M. Graham and P. O’Callaghan: Vitamins, homocysteine and cardiovascular risk. Cardiovasc Drugs Ther, 16(5), 383-9 (2002)
(9) P. J. Kelly, V. E. Shih, J. P. Kistler, M. Barron, H. Lee, R. Mandell and K. L. Furie: Low vitamin B6 but not homocyst(e)ine is associated with increased risk of stroke and transient ischemic attack in the era of folic acid grain fortification. Stroke, 34(6), e51-4 (2003)
(10) B. N. Ames and P. Wakimoto: Are vitamin and mineral deficiencies a major cancer risk? Nat Rev Cancer, 2(9), 694-704 (2002)
(11) Riggs KM, Spiro A 3rd, Tucker K, Rush D. Relations of vitamin B12, vitamin B6, folate, and homocysteine to cognitive performance in the Normative Aging Study. Am J Clin Nutr 1996; 63:306-314.
(12) Cohen M, Bendich A. Safety of pyridoxine – a review of human and animal studies. Toxicol Lett 1986;34:129– 139.
(13)Schaumburg HH, Berger A. Pyridoxine neurotoxicity. In: Leklem JE, Reynolds RD, editors. Clinical and physiological applications of vitamin B6. New York: Alan R. Liss; 1988. pp. 403–414.
(14) Joe Leigh Simpson, Lynn B. Bailey, Klaus Pietrzik, Barry Shane, Wolfgang Holzgreve, Micronutrients and women of reproductive potential: required dietary intake and consequences of dietary deficiency or excess. Part I – Folate, Vitamin B12, Vitamin B6
(15) Vrolijk MF, Opperhuizen A, Jansen EHJM, Hageman GJ, Bast A, Haenen GRMM. The vitamin B6 paradox: Supplementation with high concentrations of pyridoxine leads to decreased vitamin B6 function. Toxicol In Vitro. 2017 Oct;44:206-212 (16) Ubbink JB, Serfontein WJ, Becker PJ, de Villiers LS. Effect of different levels of oral pyridoxine supplementation on plasma pyridoxal-5′-phosphate and pyridoxal levels and urinary vitamin B-6 excretion. Am J Clin Nutr. 1987 Jul;46(1):78-85.


